Disparities in Trends of Gastroenteropancreatic Neuroendocrine Tumor Incidence
To the Editor Accurate identification of significant sex and age disparities in the trends of gastroenteropancreatic neuroendocrine tumor (GEP-NETs) incidence are crucial for informing public health intervention and policymaking. A recent analysis by Abboud and colleagues reported an increasing inc…
Physician Suicide and Associated Features—What Defines a Physician?
To the Editor Makhija et al defined the national incidence of physician suicide and associated features in a well-detailed study of the National Violent Death Reporting System data and death certificates. This is an important problem for the profession, and additional data and insights are valuable…
Estimating Treatment Effects From Observational Data
This Viewpoint describes the target trial emulation approach and the importance of it being used thoughtfully and correctly.
Dysbiosis exists in unaffected relatives of inflammatory bowel disease (IBD): emphasising the critical phases in the developmental trajectory of gut microbiota
Inflammatory bowel disease (IBD) has emerged as a global disease, affecting individuals of every ethnicity and age groups worldwide.1 It is broadly accepted that the greatest single risk factor for the development of IBD is having an affected family member.2 First-degree relatives (FDRs) of patient…
Is the green mark really recyclable?
I read the paper by López-Muñoz et al1 on ‘Life cycle assessment of routinely used endoscopic instruments and simple intervention to reduce our environmental impact’ with great interest. The green mark setting for parts that do not come into contact with the endoscope’s operating channel is a very …
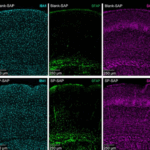
Glucocorticoid receptor suppresses GATA6-mediated RNA polymerase II pause release to modulate classical subtype identity in pancreatic cancer
Background
Pancreatic ductal adenocarcinoma (PDAC) is a highly lethal cancer with a 5-year survival rate of 12%. It has two major molecular subtypes: classical and basal, regulated by the master transcription factors (MTFs) GATA6 and Np63, respectively.
Objective
This study sought to uncover the tr…
Correction: Fatty acids promote fatty liver disease via the dysregulation of 3-mercaptopyruvate sulfurtransferase/hydrogen sulfide pathway
Li M, Xu C, Shi J, et al. et al Fatty acids promote fatty liver disease via the dysregulation of 3-mercaptopyruvate sulfurtransferase/hydrogen sulfide pathway. Gut 2018;67:2169–80.
This article has been corrected since it was first published. During the integration of data and preparation of final …
Centri per la cura dei tumori ginecologici – Lombardia
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Lombardia, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Piemonte
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Piemonte, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Campania
Centri specialistici per la cura dei tumori ginecologiciAvellino – Ospedale San Giuseppe Moscati Ambulatorio Ostetricia e Ginecologia Indirizzo: Città Ospedaliera – Contrada Moretta...
Centri per la cura dei tumori ginecologici – Puglia
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Puglia, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Toscana
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Toscana, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Sicilia
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Sicilia, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Veneto
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Veneto, per la cura dei tumori ginecologici, che offrono un approccio multidisciplinare,...
Centri per la cura dei tumori ginecologici – Friuli Venezia Giulia
Centri specialistici per la cura dei tumori ginecologiciElenco dei centri specialistici della Regione Friuli Venezia Giulia, per la cura dei tumori ginecologici, che offrono un approccio...